Defining Styles
Cataract
April 7, 2016

My cataract surgery went very well. For those who will undergo it, here are a few details.
From a certain age onward, vision deteriorates as the lenses gradually become opaque. The defective lens is then removed and replaced with an implant. During the operation—which does not require hospitalization—drops are used to dilate the iris, while others make the cornea insensitive. A drip is set up to inject a mild anesthetic just before surgery, which does not reach unconsciousness. The patient’s head, lying down, is immobilized with adhesive tape, and they are asked to look straight ahead.
The surgeon then opens the cornea with a 2 mm incision through which a source of ultrasound is introduced. This breaks down the lens, fragmenting it (the technical term is "emulsify"). Alternating operations, the surgeon attacks the lens and aspirates the fragments until the chamber is completely emptied. This chamber is separated from the vitreous humor—contained within the eyeball—by a transparent membrane.
During surgery, patients are asked to "fixate on the light." But very quickly, as the lens is fragmented and the patient perceives the outside world only through these fragments, they no longer see one light but several.
The surgeon then inserts the implant, rolled up inside a tube the diameter of a straw. To do this, the implant—equipped with shape memory—is expelled and immediately unfolds. It takes the form of a lens with two legs that deploy in an eccentric motion. These legs are designed to hold the implant in place within its future housing, which previously accommodated the defective lens.
The patient remains under observation for one hour until the effects of the anesthetic wear off. Personally, I returned home by bus from Aix to Pertuis, though accompanied by my wife.
No stitches are needed. The cornea heals itself within a week at most. The doctor supports healing with antibiotic and anti-inflammatory drops. DIY work is prohibited during this period (see below).
When cataract surgery becomes necessary, choose a good surgeon. The procedure to destroy and evacuate the lens takes about fifteen minutes, and implant placement takes just a few more minutes. This brevity tempts some less scrupulous surgeons to "boost numbers" by multiplying brief operations, often carelessly performed due to fatigue and lack of attention. A friend of mine, six months ago, became a victim of one of these overzealous surgeons. The surgery is simple, provided it is done with a steady hand. Otherwise, the surgical error lies in poorly positioning the implant—done hastily. In such cases, reoperation is required. Thus, in every region, there is a surgeon who corrects the x percent error made by colleagues.
Since I had to choose, I preferred dealing directly with this one.
Cataracts have plagued humanity for millennia. If left untreated, they gradually progress until total lens opacity—i.e., blindness. Before implants were available, doctors throughout history, including ancient Egyptians, performed a drastic operation: inserting a needle into the eye and pushing the lens downward into the vitreous humor. The patient did not regain normal vision, but at least could perceive light again.
The idea of implant placement emerged shortly after World War II when surgeons treating fighter pilots whose cockpit plexiglass had shattered noticed that these pilots had retained fragments in their eyes for years without discomfort. The conclusion was that the eye tolerates objects made of this material very well, without triggering rejection mechanisms.
Implant placement techniques matured in the early 1970s. Since then, they have been refined. Instead of extracting the lens from its housing—which required an incision over 10 mm—ultrasound destruction allowed limiting the incision to just 2 mm. Additionally, the emergence of shape-memory materials enabled presenting the implant rolled up in a tube, further reducing the incision size.
Technology advances worldwide across all fields. Too often, the focus is military or exclusively profit-driven: GMOs, unnecessary and even harmful vaccinations, agri-food industry excesses, etc. Here, however, we have something that aims solely to improve human living conditions—and incidentally increases life expectancy. Not being able to see means retreating inward, losing the ability to read, to communicate. Thus, depression and a shortened path toward death.
For two weeks, I built a wooden model illustrating my vision of how the Great Pyramids might have been reconstructed. I had to saw sticks and battens until I developed a stiff neck. But it turned out to be quite an impressive object.

I will now be able to finish the comic strip I started. I plan to complete this online presentation with the article I sent in 2004 to the Bulletin de l'Institut Français d'Archéologie Orientale, the classic "BIFAO," which rejected it on the grounds of "lack of philological data" (in other words, "on what papyrus did you find this?"). We’ll see if I have better luck this time. To that end, I created a PDF describing in 95 images how to build this model, so enthusiasts can recreate it at home using 2 cm x 2 cm sticks and 2 cm x 4 cm battens. Just add glue and a guide for making 90° and 45° cuts. I won’t expect Egyptologists reading the article to do the same—though only by handling the object can one truly understand it.
This is, therefore, a stone spiral ramp made of the same material as the final facing (fine Tura limestone), enabling centimeter-precise guidance of the work. This ramp could then carry loads of up to 60 tons (the heaviest monoliths, such as those forming the ceiling of the King’s Chamber in Khufu’s pyramid). What’s interesting is that this ramp is built from a standardized "pyramid construction kit" inherited by each pharaoh, greatly accelerating the work. When transforming this ramp into the final facing, cutting is limited to removing triangular blocks—plentiful at the Giza site (I took these photos myself a few years ago).
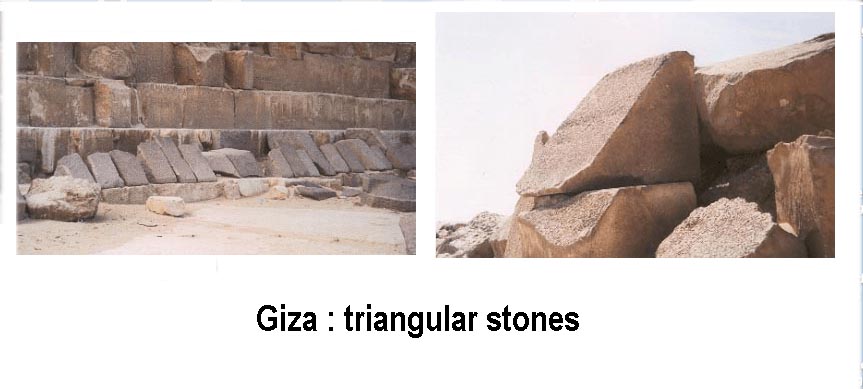
Thus, 75% of the stone placed constitutes... the facing. The next 20% go toward the kit for the next pyramid, and only 5% are these unusable triangular stones. Finally, a finishing touch by sanding remains.
It’s a pity we no longer build pyramids today. Otherwise, I think I’d now be fairly capable of leading such a project. At any rate, with the model now proudly displayed in my living room, I had great fun making it. Of course, it would have looked more elegant with fine woods and been more precise with a band saw. Let’s just say it’s a "Mr. Handyman Pyramid."
After healing from cataract surgery and completing the comic strip, back to cosmology and astrophysics.