Should prostate cancer be screened for?
A manifesto by doctors who declare themselves against screening for prostate cancer.
May 2, 2010
Dr. Dominique Dupagne:
http://www.dailymotion.com/video/x6vxfp_le-depistage-du-cancer-de-la-prosta_lifestyle
Dr. Dominique Dupagne is part of a group of 80 doctors who have decided to express their opinion on the screening of prostate cancer through PSA testing and rectal examination. I completely agree with what he says in this video, which I strongly recommend my male readers to watch, despite its length and lack of illustrations. I will continue with my own comments.
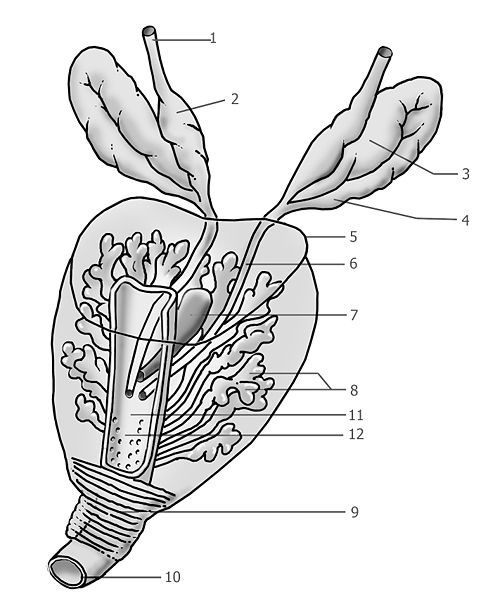
The prostate is an organ, related to the male uro-genital system. Few men know what it is, where it is located, and what its functions are until it reveals itself by causing some discomfort. First, a bit of anatomy:
I have intentionally enlarged the Wikipedia image to clearly indicate the details.
In gray, the skeletal elements, the bones. The pelvis, for both men and women, is shaped like a kind of container, to hold the internal organs, which would tend to drop when standing. At the back, the terminal part of the spine is visible: the sacrum.
The bladder, partially resting on the front of the body on the pubic bone arch, is clearly visible. Just below it is a gland, called the prostate. It is traversed by different channels.
-
The first is the urethra, which carries the urine from the bladder.
-
In this urethral channel, several substances are poured. On the right are the seminal vesicles, which secrete a liquid that is one of the main components of semen. A liquid from the testicles, containing sperm, is also poured into this.
-
Below the prostate is the Cowper's gland, which secretes a lubricant, which is emitted when the man is aroused. The seminal fluid flows through the ejaculatory ducts, which pass through the prostate. It is the contraction of the prostate that causes ejaculation.
Below is another view of the prostate, the ducts, the urethra, and the location of the urethral sphincter:
Let's move on to the behavior of the prostate. Very small at birth, it increases in size during puberty, and in adulthood has the size of a walnut. Then, as age comes, a benign tumor develops within it, called an adenoma, which increases its volume. This benign evolution affects 80% of men over 50 years old. This tumorous evolution can appear in the form of several nodules. This growth compresses the urethral canal, through which urine flows. Doctors can then prescribe a comfort medication, which alleviates or eliminates this inconvenience, Xatral, or its generic version. It is reimbursed by the French Social Security.
This same prostate can be the site of more or less recurrent inflammations, but without particular danger, called prostatitis.
It is possible to measure different antigens generated by the prostate, including the PSA (Prostate Specific Antigen). The amount of PSA produced, which is measured by a simple blood test, depends on different factors. For example, the size of the prostate. This production increases during an infection, such as a urinary tract infection. But it also increases when a cancer develops within the prostate. Its detection by imaging is problematic because it is difficult to distinguish between a cancerous tumor and a benign tumor, which is common and practically automatic in men over 50 years old.
Doctors, and urologists, can then prescribe a biopsy, which can be performed under general or simply local anesthesia. In this procedure, the practitioner inserts a gun-like device through the anus that sends a metal probe toward the prostate, which, when retracted, collects a certain amount of cells. During this biopsy, the urologist, guided by an ultrasound view, makes about ten "shots". These samples are then analyzed and cancerous cells are searched for.
When the PSA level remains high, the urologist may estimate that his examination missed the developing cancerous tumor, and he may wish to repeat the procedure. I have known patients who underwent this up to ten times, until the final detection of a small cancerous tumor that had escaped previous examinations. The urologist had thus turned their prostate into a sieve, with more than a hundred exploration points.
Men die every day from prostate cancer (this was the cancer that took Mitterand). The tumor can send metastases to nearby lymph nodes or to the bones. When these cancers progress, bone metastases are the source of intense pain that quickly leads to palliative treatment with opiates (morphine).
Before this metastatic progression occurs, the urologist can consider several treatments. The most recommended:
-
Simple removal: the prostate and seminal glands are removed.
-
Hormone therapy
These treatments have obvious effects on sexual behavior. An operation that has affected the sphincter that blocks the urine flow, or nerves that control this sphincter, will make the patient incontinent. Damage to the nerves controlling his sexual behavior will make him impotent.
As Dr. Dupagne clearly states, our body constantly produces cancer cells, which are eliminated by our immune system. The prostate is a site of dormant, small cancers (the size of a grain of rice, they can escape the biopsy's exploratory shots). They have a very slow evolution. Statistics indicate that half of men over 60 have prostate cancer. This proportion increases with age. When patients die at 90 years old from other causes, if an autopsy is performed on them, a prostate cancer is found, which continued its evolution quietly, without metastases.

Excerpt from the Wikipedia dossier on prostate cancer, which confirms Dr. Dupagne's statements:
The difficulties of prostate cancer screening are multiple, and the unresolved issue is to differentiate between potentially progressive and dangerous forms from the quiescent forms that probably affect one out of two men in old age.
Current screening is based only on two exams that are inherently very insufficient (in the context of this screening): PSA level testing and rectal examination (the latter can detect a nodule or localized hardening). These exams have low specificity and sensitivity. More recently, an analysis of the PCA3 gene, followed by biopsies, has been proposed.
Screening campaigns certainly detect a large number of "carriers" of cancer cells, but the risk of "overtreatment" and related morbidity remains difficult to evaluate. Moreover, there are conflicting data regarding a possible decrease in mortality or an improvement in the quality of life for those detected and treated surgically or specifically managed.
I refer the reader to Dr. Dupagne's video presentation. What he cannot say and what must be added is that these screening operations, and especially the biopsies, "drive the business." Hence an intensive campaign, funded by pharmaceutical companies, to promote this kind of diagnosis and sell products, tests, and equipment.
mammography ****
May 5, 2010:
Noted by a reader, Blanche Monavar, 89 years old:
Controversy around breast cancer screening by
(radiological examination)
Mammography by radiological examination. Above, the source of X-rays